COPD Support Ireland & The Chronic Disease Management Programme
Written by Deirdre Garvin, Respiratory CNS, Mayo University Hospital/Board Member, COPD Support Ireland
The health and life expectancy of the Irish population has improved, and with this comes a greater need for healthcare in chronic disease in Ireland.
The Slaintecare report (2017) of the Oireachtas Committee on the Future of Healthcare set out the vision for health service reform to improve the health of the nation. 7 The aim is to provide a universal healthcare system and to move care delivery from the acute health care setting, which is unsustainable, to care closer to home which includes promoting health and wellbeing and meets the patients’ needs in a fair and equitable way. 4,5,7
The integrated model of care for the prevention and management of chronic disease (IMPCD) is the essence of the national framework for integrated prevention and management of chronic disease in Ireland 2020-2025 and details how end to end care will be available in Ireland. 4,5
Integrated care is the process of providing this Slaintecare vision for patients and integrated care has been shown to improve care by meeting population health need. 4,5 Research shows patients with chronic diseases, including respiratory, when managed and cared for in primary care with good governance and clinical leadership have improved care and outcomes than if provided in acute services. 7
Integrated care for chronic disease is care provided at the lowest level of complexity, close to home with services to support and empower individuals to optimise their health and minimise risk factors for developing or progression of their chronic disease. 4,7
Health promotion and education by preventing illness in the first place and preventing progression is in line with Healthy Ireland policy which seeks to improve health through preventive strategies and supporting people to live healthier lives, which in turn reduces demand for hospital care. 2,4,7
The framework is the mechanism of delivering care, which is person centred, holistic to the person and preventative. 19 The various models of care and national clinical care programmes including the COPD model of care, have all adapted an integrated approach and are developing care around the framework which is line with policy. 3,4,5,7
Slaintecare and the integrated framework detail the health reform including the development of 6 Regional Health Areas (RHA,). These are then further broken down into 96 Community Healthcare Networks (CHNs). 4,5
CHN’s are geographical based units which serves a population of approximately 50,000 and three CHN’s will be served by a specialist ambulatory care hub for chronic disease serving a population of approximately 150,000. An ambulatory care hub will be a clinical site away from the hospital setting which will support access to diagnostic, specialists’ services and specialists’ opinions. Health care will primarily be delivered in the community with supports available to allow this by providing specialist care when needed within the community in chronic disease including COPD and this care will then be delivered closer to home. 4,5,7
The treatment, burden and management of chronic illnesses account for a large share of health resources, including 80% of all general practitioner (GP) visits, 40% of acute admissions, 75% of hospital bed days and accounts for poorer quality of life. 3,6,7,8,9
In the area of respiratory the true prevalence of respiratory conditions such as COPD in Ireland is unknown. It is estimated that 500,000 have COPD, however only approx. 200000 are diagnosed and many are unaware of their condition. 1,8,9 COPD is a major health burden and causes morbidity and mortality in Ireland with over 1500 deaths and 15,000 patients admitted to hospital annually. 3,8,9 Ireland has the highest rate of hospital admission with COPD of any country in the OECD. 8,11
There was considerable variability in COPD care with variation in length of hospital stay, access to diagnosis, access to Pulmonary Rehabilitation and COPD Outreach. 3
The national framework for Integrated prevention and management of Chronic diseases which includes COPD is a whole system approach to integration that incorporated population health, wellbeing, preventative, acute, non-acute and community-based services. 4,5
The framework is person centred, holistic proactive and preventative in endeavours to make care accessible and equitable for all. It will improve care for our COPD patients by providing access to diagnostic, specialist expertise, pulmonary rehabilitation, and COPD outreach across the country. 3,4,5,10
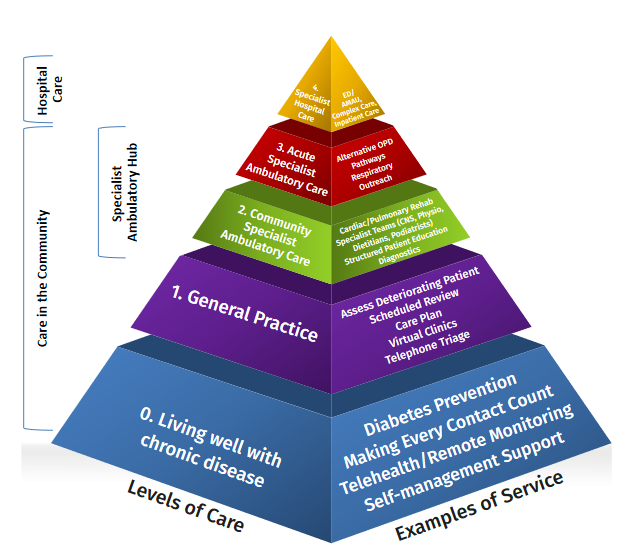
The national framework for the integrated prevention and management of Chronic Disease in Ireland along with the accompanying 10 step guide document details how care will be delivered and details the 5 levels of care as seen in below diagrams. 4,5
The MOC for COPD takes a holistic, person centred and life course approach to the provision of services. 3,10 It reflects the principles of integrated care which in essence is to provide patients with the right care at the right time by the right team in the right place and to reduce inequalities and describes what services will be provided at each level of care. 3
It is anticipated that patients through their journey will move through the levels of care, however primarily care will be provided in the community and a greater emphasis now is on primary prevention, health promotion and population health. 3,10
Through early identification of risk factors through professionals using, Making every Contact Count (MECC) this will allow early detection and diagnosis, therefore appropriate management and in turn prevent or delay the onset of COPD. 3,5,10
This will improve care for all patients across the levels of care as appropriate, allowing for specialist inpatient, specialist ambulatory care, specialist support to General Practice and chronic disease prevention and management in primary care, all supported by patient self-management with the aims of saving lives of people with COPD and in turn the reduction of hospitalisations and morbidity of COPD patients. 3,4,5,10
The model of care details the 4 levels of service and level 0 care is included in the resource document on COPD integrated Service model.
In general terms level 0 care is about keeping communities healthy and to keep those with chronic disease living well. 3,4,10 The integrated framework describes how services are being developed to support and empower individuals living in our communities to prevent and manage their chronic diseases. 4,5 Services include education, support to manage their diseases and each RHA and CHN is tasked with mapping all services available including HSE funded, voluntary and community.
This allows development of services that are lacking but also making best use of services that are in fact available. However, it is of paramount importance that all health care professionals (HCP’s) are aware of available services and can sign post patients and their families to these services The making every contact count (MECC) as a health promotion ensures health promotion is a focus of each HCP and patient encounter and should be a focus for us all.
This includes each patient encounter albeit in the GP’s surgery during an acute illness, during a structured chronic disease review, or a pharmacy visit. This requires staff to be aware of what’s available to support patients in their communities.
Level 0 care available and appropriate for COPD patients
• Living Well with chronic disease programme
• Self-Management programme
• Stress management Programme
• COPD Support Ireland Website
• Social Prescribing,
• Flourish programme
• Sing strong programme
• Making every Contact count
• Tele-Health, remote monitoring
• COPD support Groups
• COPD support Ireland nurses phone line
• Smoking Cessation services
COPD Support Ireland (COPDSI) was established in 2013 as Irelands National COPD Support and Advocacy organisation and has established over 35 communitybased COPD exercise and peer support groups across the country.
It supports patients and their families living with COPD throughout Ireland through various channels. The work of COPD Ireland supplements the work of the integrated framework for chronic disease and the model of care and can support patients and their families across all the 5 levels of care.
Patients can access information and services throughout their disease trajectory from diagnosis onwards. COPDSI work complements the work of the integrated care programme and model of care for chronic disease as much of its work focuses on providing services that supports those to live well and education on self-management. Equally it is a great source of knowledge for those who are undiagnosed and may want to learn a bit more about the disease and then seek help. Those who seek advice and are supported through various channels often are better equipped to manage their condition and COPDSI can support this.
It is important that those of us working in healthcare are aware of supports available to our patients and can sign post patients and their families to the resources available. COPDSI has recently sent correspondence to Respiratory physicians of the valuable services it provides to help support their patients and this in turn can support the health service.
Services provided by COPDSI include:
COPD Adviceline 1800 83 21 46 is a HSE funded freephone service, delivered with the Asthma Society of Ireland; for people who want to discuss or learn more about their COPD and its Self-Management from a specialist respiratory nurse or physiotherapist. It is a valuable resource for patients and their families to learn more about COPD.
COPD & Me Exercise Programme
COPDSI developed a community-based COPD exercise programme delivered by fitness professionals. Classes take place weekly, either virtually, or in person at a local support group location. Participation in these classes has been shown to increase exercise capacity & gait speed and to reduce anxiety. You can refer patients to the COPD & Me exercise programme through the HCP referral link on www.copd.ie
COPD & Me Book
Is a comprehensive patient information and Self-Management education Book. Designed in collaboration with the Respiratory National Clinical Programme and supported by the Chronic Disease Management Programme, this book is now available to HSE COPD services nationally during 2022. To order copies, email info@copd.ie.
Sing Strong – Singing for better Lung Health
In COPD Self-Management, airway clearance and breathing control are taught to help control dyspnoea. Sing Strong is a novel, fun and popular way to learn and implement these techniques through singing. Created by vocal coach Ms. Ciara Meade and lecturer of cardiovascular and respiratory physiotherapy, Dr. Roisin Cahalan, SingStrong is delivered virtually or in person, over 10-weeks through COPDSI.
In conclusion the rolling out of the national framework for integrated prevention and management of Chronic Disease and Model of care for COPD is a welcome development for those suffering and or at risk of developing COPD. Care and services which meets population health needs will be accessible and available and not a post code lottery service of services available in certain locations. COPDSI is a valuable resource to both HCP’s and patients and its work needs to be communicated to those who may benefit from its services.
References on request